Spondylosis vs Spondylolysis vs Spondylolisthesis
There is a growing interest in understanding spondylolisthesis and spondyloptosis. Spondylolisthesis vs spondyloptosis? Spondylolisthesis is a slipping or untoward movement of one vertebra on the other. The point to understand is that the vertebra that has slipped carries the weight with it as it slips forward. What about spondyloptosis? We think the ideal definition of spondyloptosis is when the cephalad vertebrae’s posterior superior corner is caudal to the inferior vertebrae’s anterior superior corner. It is more or less difficult to assess the anterior superior corner since the sacrum has several adaptive changes and therein lies one of the controversies with spondylolisthesis.
What is Spondylosis?
Spondylosis is a condition in which there is a progressive degeneration of the intervertebral discs leading to change in the surrounding structures. In the past this condition has been called osteoarthritis, cervical spondylitis, herniated disc, chondroma, etc., but the term spondylosis is preferable as it is a degenerative rather than a neoplastic or inflammatory condition. Healing of lumbar spondylosis requires strengthening of hip muscles which aids in recovery in the longer run.
Although it has been known for many years that lesions of the cervical spine may cause paraplegia it was not until fairly recently that the importance of cervical spondylosis in the production of symptoms was recognised. The first recorded reference to paraplegia following an injury to the cervical spine is found in the Edwin Smith Papyrus written 4,000 years ago.
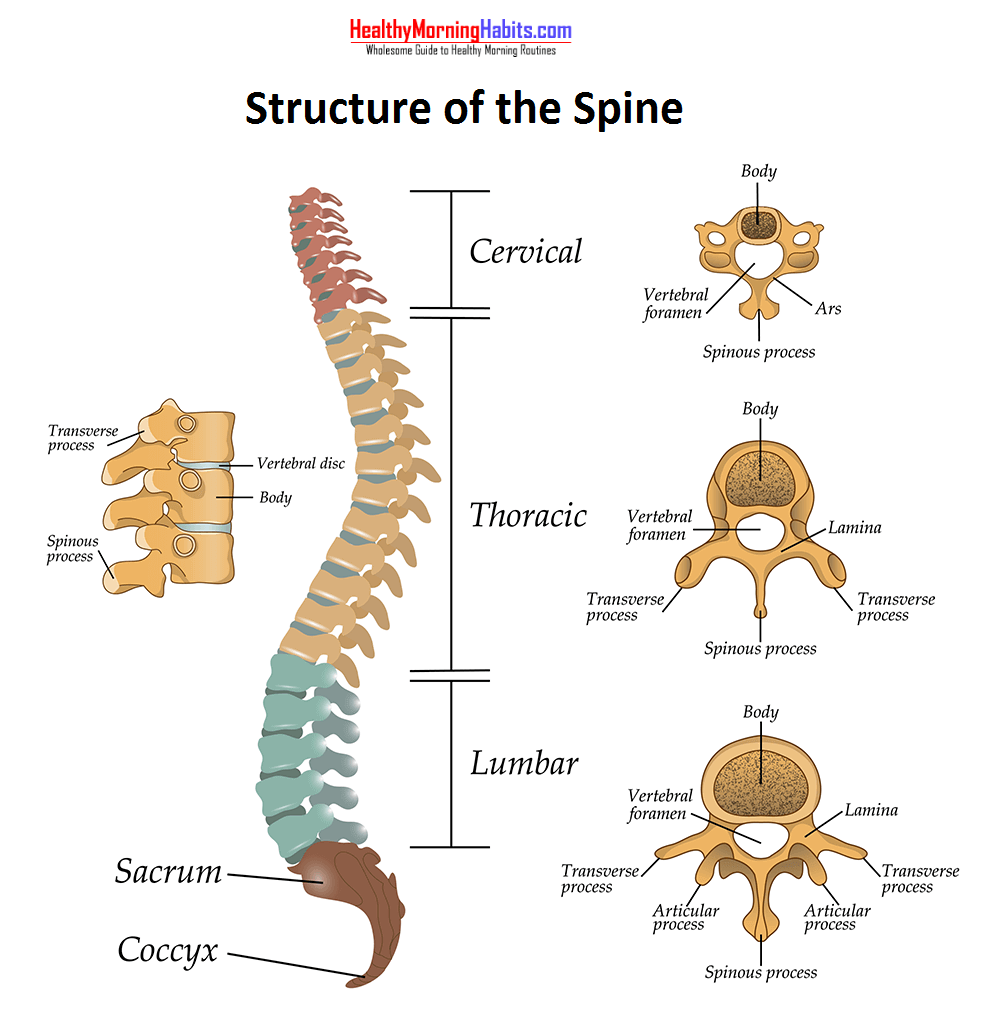
The cervical vertebrae play an essential part in the maintenance and alteration of the position of the head, and therefore, have a significant rôle in governing postural reflexes. The groups of muscles attached to this part of the spine have three main functions: movement of the head and neck, by coarse and fine adjustment; suspension and movement of the shoulder girdle and suspension, fixation and active elevation of the thoracic inlet. In addition, the vertebral canal houses the meninges and the spinal cord which is at its maximum diameter in this region. The vertebral arteries are supported and constantly subjected to movement in the rigid bony foramina transversaria. On their way to supply the contents of the posterior cranial fossa and visual cortex, these vessels also supply the vertebrae, intervertebral joints, meninges, spinal cord, dorsal root ganglia and the cervical nerve roots.
What is Spondylolysis ?
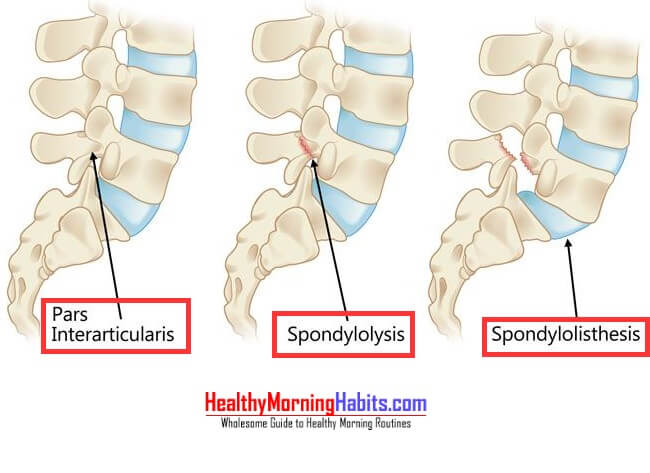
Spondylolysis is a fracture of the pars interarticularis. If the defect on the pars is bilateral, it might or might not allow slippage of the vertebra, resulting in spondylolisthesis. Mechanical and structural stress are the main cause of spondylolisthesis, which being one of the most common in the lower spine at L4 and L5. At these levels the spine predominantly carries more load than higher levels of the spine. Thus having a greater shear forces due to the lumbar lordosis. This may result in a stress fracture on the pars. Athletes tend to develop pars defects than nonathletes. Sports that includes repetitive hyperextension result in microtrauma to the pars. Some of the such aggrevating sports may include sailing, wrestling, weight lifting, American football, hurdling,pole vaulting, gymnastics,rowing, diving, volleyball, tennis, swimming, cricket, and baseball.
A quick fact:
Gymnasts are 3-4 times more likely to develop spondylolysis, and more than 2 out of every 4 American football linebackers may develop pars defect. similarly in the same sport, at the blocking position, the compression force on an average on L5 is Six to Seven times the body weight of the athlete, and the peak shear force is roughly around 3 times body weight.
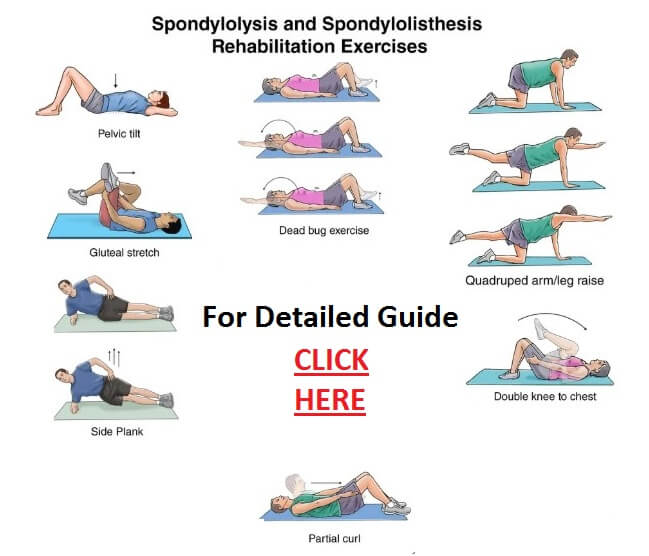
Strengthening your lower back is the key to recovery from any form of Spondylosis. We had one of our editor share his experience unlocking his hip flexors which helped him and his wife recover from lower back fatigue
Three definitions of spondyloptosis are:
- “When the L5 vertebra is completely off the sacrum.”
- “When the L5 vertebra is in front of the sacrum:’
- ”A Grade V spondylolisthesis
Spondylolysis vs spondylolisthesis vs spondylolisthesis occur predominantly in the lower lumbar spine, irrespective of the different underlying problems. Spondylolysis and spondylolisthesis usually occur in the lumbar spine at L4 and L5. The reason for this is that they carry more loads and are more susceptible to shear forces due to the lumbar lordosis. The vertebral bodies and intervertebral discs share compressive forces, and shear forces are shared by the facets, discs, and spinal ligaments.
Treatment for Cervical Spondylosis
Bed rest
Bed rest is a very effective method of treatment for this type of condition. The patient is told to lie flat in bed with only one pillow, as in the treatment of sciatica, and if the pain is severe the head may be placed between sandbags. After a period of 3 to 7 days the pain goes, this probably being due to relaxation of the spasm of the neck muscles. Following this period of rest a course of exercises for the neck and shoulders, lying flat in bed, should be given after which the patient can be allowed to get up gradually, the exercises being continued. Although bed rest has good results for spondylolysis, spondylolisthesis & spondylolisthesis it is often difficult to persuade a patient to carry out this treatment, for on the whole rest in bed is regarded by him as an unnecessarily severe treatment for pain in the arm.
Collars
Many types of collar have been recommended for treatment of cervical spondylosis but in our experience the number of patients requiring a collar is very limited, as most recover in any case in 4 to 6 weeks. The object of the collar is to limit or reduce neck movements in order to give any “inflammation” or oedema present due to spondylolysis, spondylolisthesis & spondylolisthesis, a chance to subside. It is also thought that trauma to the cervical cord by the cervical spondylotic bosses or bars may be minimised by wearing a collar because excessive or even normal neck movements might traumatise the cord against these or the ligamenta flava. Collars vary from the massive Minerva plaster, which immobilises the head and neck, to light collars made of felt, sorbo, rubber or even paper. The length of time that a collar should be worn is often disputed. As the osteophyte will either remain unchanged or increase slightly in size it would be logical to suggest that it be worn for life. Most people, however, feel that in practice if there has been no good result from wearing a collar for 3 to 4 months it should be discarded. Prolonged use of a collar may so weaken the cervical muscles that the patient becomes unable to do without it.
Traction
Traction has been a popular treatment of cervical spine lesions for many years. In acute disc lesions and in cases of root compression where pain is the main complaint and the underlying pathological changes are minimal, traction is often helpful but it is of very little value in patients with acute radiculopathy (Type 2) or chronic radiculopathy. The main effect of traction is to overcome spasm of the neck muscles, and though the initial effect may be good the symptoms are likely to recur. Traction is generally preceded by heat and gentle mobilising exercises. These exercises are often only gentle active movements, but sometimes passive movements and manipulation may be used as well. Traction may be applied in several ways for spondylolysis, spondylolisthesis & spondylolisthesis. It is best given by means of a head halter, weights and a pulley, the patient lying on a plinth with the pulley fixed at a suitable height at one end. A sling is used and the head supported on a pillow. It is usual to begin traction with 10 lbs. for 20 minutes and increase up to 15 lbs. for 30 minutes by the second or third day; 10-12 lbs. is sufficient for a small woman whilst a large man may require 20-25 lbs. A limiting factor is aching in the temporomandibular joints due to the thrust from the chin-strap of the halter. Almost all patients can tolerate up to 15 lbs., but a substantial proportion find 20 lbs. too much. The direction of pull requires attention. If a patient has pain and stiffness in the neck with no referred pain the direction of traction should be straight, with perhaps a slight tendency to flexion rather than extension. Patients with referred pain should be tested to find out if any position increases the referred pain and the direction of pull then arranged so that it is in the opposite direction, i.e. if referred pain is increased by combined extension and tilting or rotation, the pull should be in some degree of flexion and tilting or rotation to the opposite side.
This assessment for spondylolysis, spondylolisthesis & spondylolisthesis needs to be repeated each time the patient attends because the position causing maximum referred pain is apt to vary. If the neck is over-extended there will be a pull on the trachea and the oesophagus, and extension is the position in which damage to the spinal cord is most likely to occur. Vertical traction may also be applied by means of a Sayre sling with the patient in the sitting position. When head traction is used it should be applied slowly, because sudden jerks or twists of the head may cause acute compression of the spinal cord the results of which could be fatal. Traction should be abandoned if it causes exacerbation of symptoms.
Manipulation of spine
Manipulation has been described as “a forcing movement with special purposes other than direct increase in the range of movement of a joint”. In the cervical spine its main use is to reduce an intra-articular displacement or mobilise the zygapophyseal joint and the neuro-central joint. Following manipulation for spondylolysis, spondylolisthesis & spondylolisthesis there may be an immediate relief of pain especially if this is due to spasm of the neck muscles. The effect is unlikely to be permanent. When there are signs of cord compression manipulation is contra-indicated as the liability of further cord damage is considerable.
Other forms of physiotherapy
These include heat and diathermy, massage, active and passive movements. Heat and diathermy are usually used to relax the muscles before active exercises or traction are applied. They are useful in diminishing the pain which is often the main symptom. Many patients who develop symptoms of root and cord involvement in middle and later life are found to have sagging of one shoulder or some other asymmetry of the shoulder girdle. Frequently their posture is bad and often they have an upper dorsal kyphosis. A course of active exercises for the neck and shoulder girdle muscles along with treatment for spondylolysis, spondylolisthesis & spondylolisthesis may cause a marked improvement especially when combined with heat and diathermy. It is possible that in these patients the poor tone of the muscles causes an increased strain on the nerves and ligaments and so leads to symptoms. To be effective, the spine exercises should be done for 10 minutes three times a day. Passive movements are sometimes used to “free adhesions” but where spondylotic changes are well marked this may be a dangerous procedure. If there is any degree of vertebro-basilar insufficiency strong passive movements of the neck may well cause giddiness and in these circumstances should not be done.
Radiotherapy
Deep X-ray therapy has been used in the treatment of cervical spondylosis but there is no good evidence that this shortens the natural course of the symptoms.
References:
- Analysis of cervical spine curvature in patients with cervical spondylosis
- Anterior cervical decompression and fusion for cervical spondylosis using vertebral grafts obtained from the fusion site. Technical advantages and follow-up results.
- Cervical spinal cord injuries in patients with cervical spondylosis.
- Cervical spondylosis and cysts of dorsal root ganglia.









